StudentShare

Our website is a unique platform where students can share their papers in a matter of giving an example of the work to be done. If you find papers
matching your topic, you may use them only as an example of work. This is 100% legal. You may not submit downloaded papers as your own, that is cheating. Also you
should remember, that this work was alredy submitted once by a student who originally wrote it.
✕
Free
Data on Predictors of STDs - Report Example
Summary
The paper "Data Report on Predictors of STDs" discusses that future research should explore sexual networks of Pacific and Asian Islanders, including the extent of concurrent sexual relationships and network exposure in shedding light on pathways and mechanisms of STD acquisition…
- Subject: Health Sciences & Medicine
- Type: Report
- Level: High School
- Pages: 5 (1250 words)
- Downloads: 0
- Author: lbosco
Extract of sample "Data on Predictors of STDs"
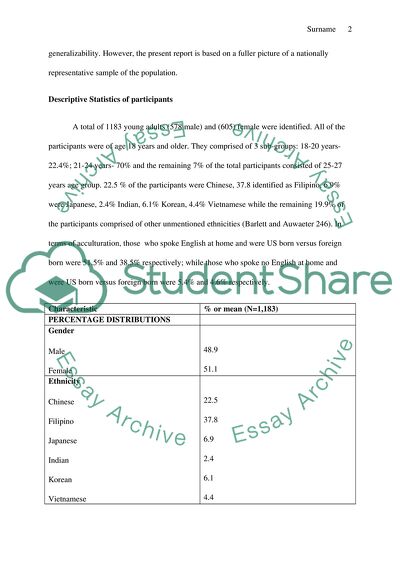
Data report on predictors of STDs Background STDs are among the most common infectious diseases in the United s.The data for this report was obtained from the National Longitudinal study of Adolescent Health, wave 3.the bivariate analyses of the relationships between explanatory variables and STD status utilized a chi-square test. Models of multiple logistic regression analysis included ten of the bivariate analyses in identifying the factors associated with STDs. The sample under study encompassed Pacific and Asian youth of middle and high school; 578 were male and 605 female, aged 18 years and older. Logistic regression analysis was utilized in assessing the factors associated with the history of an STD (Barlett and Auwaeter 235).This report’s purpose is the analysis of the various predictors of an STD. With the high population growth rate of the two islander groups in the United States, knowledge about the factors associated with STDs still remain sketchy. Investigations of STDS and HIV among this population have had the largest focus on men having sex with other men. However, researches have paid insufficient attention to Pacific and Asian women and their STD vulnerability. Previous studies used smaller samples, focused on a single ethnicity, employed limited analysis of statistics and were reliant on regional other than national samples. This resulted in lacking generalizability. However, the present report is based on a fuller picture of a nationally representative sample of the population.
Descriptive Statistics of participants
A total of 1183 young adults (578 male) and (605) female were identified. All of the participants were of age 18 years and older. They comprised of 3 sub-groups: 18-20 years-22.4%; 21-24 years- 70% and the remaining 7% of the total participants consisted of 25-27 years age group. 22.5 % of the participants were Chinese, 37.8 identified as Filipino, 6.9% were Japanese, 2.4% Indian, 6.1% Korean, 4.4% Vietnamese while the remaining 19.9% of the participants comprised of other unmentioned ethnicities (Barlett and Auwaeter 246). In terms of acculturation, those who spoke English at home and were US born versus foreign born were 51.5% and 38.5% respectively; while those who spoke no English at home and were US born versus foreign born were 5.4% and 4.6% respectively.
Characteristic
% or mean (N=1,183)
PERCENTAGE DISTRIBUTIONS
Gender
Male
Female
48.9
51.1
Ethnicity
Chinese
Filipino
Japanese
Indian
Korean
Vietnamese
Other
Age
18
19
20
21
22
23
24
25
26
27
Acculturation
Speak English at home, US born
Speak English at home, foreign born
Speak no English at home, US born
Speak no English at home, foreign born
Binge drinking in the last 12 months
Yes
No
Condom used at last sex
Yes
No
Ever paid for sex
Yes
No
Ever been paid for sex
Yes
No
Had sex before age 15
Yes
No
Had 1 sex partner in past 12 months
Yes
No
Total
Means
Health Belief Model
Perceived Susceptibility
Perception of responsiveness to treatment
Perception of relationship consequences
External cues to action
Internal cues to action
22.5
37.8
6.9
2.4
6.1
4.4
19.9
0.4
8.3
13.7
16.1
18.8
19.0
16.7
5.8
1.1
0.1
51.5
38.5
5.4
4.6
66.8
33.2
74
26
3.5
96.5
2.8
97.2
11.9
88.1
67.7
32.3
100
1.20(0.59)
4.13(1.12)
4.51(1.03)
3.98(1.11)
4.17(1.05)
Group comparisons
Overall, the respondents susceptibility to STDs was low (mean, 1.2 on a scale of 1-5;however,there was a statistically significant difference between past STD history and perceived susceptibility, t(df)=5.39) while their perceived consequences of STDs for relationships was high at a mean of 4.1 on a scale of 1-5; and t-value (t(df)=3.19) (Barlett and Auwaeter 288). Additionally, the respondents expressed a strong belief of the response of STDs to treatment, at 4.5 on a scale of 1-5 and (t (df) =2.57).
Associations
Gender disparity was a significant influence on STD acquisition. Thirteen percent of young women and four percent of young men reported history of an STD (p= 0.0001). Young women were more likely than young men to have had an STD; odds ratio-4.1 (Barlett and Auwaeter 314). Indians than Filipino’s were more likely to have an STD history (odds 8.4). Respondents ever been paid for sex and those with more than a sex partner 12 months before the interview, with increased odds of STD history at (4.7 and 4.5), respectively.
Higher-order Analyses
In the model of multiple logistic regression, Several risk behaviors and most constructs of the Health Belief Model were associated significantly with STD diagnosis at the level of the bivariate. 9% reported ever been paid for sex with a significant influence on STD acquisition, (f (df) =2.7); odds ratio 4.67. 31% had sex prior to age 15(f (df)=534) while 55% had multiple partners in the past 12 months prior to the study (f(df)=12.1); odds ratio 2.52 (Barlett and Auwaeter 321). Those participants with STD history compared with those without perceived themselves as highly susceptible to STDs. The perceived susceptibility was significant marginally in the model of the multivariate (p=0.7), but significant in missing data analyses (p=0.0004).
Graphs
Fig1. Influence of Gender on STD acquisition
Fig2 influence of ethnicity on STD acquisition
Fig3-Influence of Age on STD acquisition
Fig4-Percentage of Asian and Pacific Islander young adults who had had selected STDs
Interpretation
Young women were more likely than young men to have had an STD. Additionally, Indians than Filipino’s were more likely to have an STD history. Moreover, the respondents who have ever been paid for sex and those with more than a sex partner 12 months before the interview had increased odds of an STD history (Barlett and Auwaeter 349). Furthermore, two of the Health Belief Model constructs were associated with STD history. The more the perception of respondents on STD responsiveness to treatment, the higher their rates of having had an STD diagnosis and the more the belief that STDs affect relationships negatively, the lower the odds of having had one.
The existing literature gives insight into contextual and behavioral factors which influence Pacific and Asian Islanders. Adolescents and young adults tend to have a lower risk of getting STDs because few of them engage in sexual activity. However, for those who were sexually experienced, report a similar level of sexual activity as the adolescents of other races; with similar age at first sex and the probability for multiple partners. Gender disparity among Pacific and Asian Islanders can be explained in the context that the women have broader and racially diverse sexual networks than the men. Moreover, the level of acculturation had no significant association with STDs even at the level of the bivariate. (Barlett and Auwaeter 354). It is therefore likely that with age and longer stay in the US, away from family, their original practices and beliefs became diluted by the dominant culture. In elucidating effects on STD diagnosis of acculturation, recent immigrants and their children, with lower acculturation levels should be recruited for the study. Some health beliefs about STD severity were associated with presence of STD- treatment responsiveness and relationship consequences. Belief on the unresponsiveness of STDs to treatment will aid in reducing acquisition of STDs, since it is associated with fear and threat.
The Add Health study based on this report is a longitudinal study with many years between data collection waves. Loss to follow-up of data will thus inevitably occur. The outcome variable on STD history had its basis on self report. The approach used could be less than the ideal due to the probability of measurement error which stems from the false reports of the diagnosis of participants. Moreover, Add Health didn’t differentiate STDs due to sexual intercourse from those resulting from other means. Albeit the use of the Health Belief Model as a guide, its limitations have to be noted when utilized on adolescents (Barlett and Auwaeter 362). Criticism on the model includes lack of incorporating emotional factors, peer group influences and cognitive level factors which affect the decision-making ability in relation to personal risk objective assessment. However, the strong emphasis of the model on perceptions is a key influence on adolescent behavior.
Conclusion
Findings from the report have implications for policy and practice. It is essential to raise public awareness of STD risks particularly among young women. Future research should explore sexual networks of Pacific and Asian Islanders, including extent of concurrent sexual relationships and network exposure in shedding light on pathways and mechanisms of STD acquisition. Provision of STD education and encouraging the development of protective sexual behaviors should be conducted among the adolescents. Considering the fact the exchange of money for sex was a significant influence in this study, those communities with large sex workers should be a target. Interventions for Pacific and Asian Islanders should build on the belief of perceived STD severity. STDs among Pacific and Asian Islanders should be seen within cultural and social context where they live. Successful interventions for Pacific and Asian Islanders should include long-term solutions to risky sexual behavior problems.
Works Cited
Barlett, John and Auwaeter, Paul. The ABX guide: Diagnosis and treatment of infectious diseases. New York: Thomson PDR, 2005. Print.
Read
More
sponsored ads
Save Your Time for More Important Things
Let us write or edit the report on your topic
"Data Report on Predictors of STDs"
with a personal 20% discount.
GRAB THE BEST PAPER
