StudentShare

Our website is a unique platform where students can share their papers in a matter of giving an example of the work to be done. If you find papers
matching your topic, you may use them only as an example of work. This is 100% legal. You may not submit downloaded papers as your own, that is cheating. Also you
should remember, that this work was alredy submitted once by a student who originally wrote it.
✕
Free
Obesity in Children - Literature review Example
Summary
The paper "Obesity in Children" highlights that obesity is a growing cause of concern in both developed and developing countries. It is however a preventable issue. Therefore, large-scale lifestyle, dietary and behavioral changes need to be implemented to lower the incidence of obesity…
- Subject: Health Sciences & Medicine
- Type: Literature review
- Level: Undergraduate
- Pages: 10 (2500 words)
- Downloads: 0
- Author: greenholtleonor
Extract of sample "Obesity in Children"
Obesity in Children Schools Number and of (e.g., October 12, Obesity in Children (Literature Review)
Introduction
The statistics on childhood obesity are alarming. According to reports by the World Health Organization (WHO), the number of overweight children below five years of age, in the year 2010, was over 42 million and around 35 million of these were from developing countries (WHO, 2014)! In the past thirty years, childhood obesity has more than tripled in adolescents and doubled in children (CDC, 2013). The percentage of obese children in the 6-11 years age group in the United States increased from 7% to 18% from 1980 to 2010 (CDC). Over the same period, percentage of obese adolescents in the 12-19 age groups increased from 5% to 18%. Childhood obesity is among the most serious public health issues of the twenty first century. It is a global issue. It was earlier thought to be confined to high-income developed countries but has steadily been affecting urban populations in middle and low income countries as well. Overweight and obesity in children are likely to persist in adulthood. Obesity is the fifth leading risk factor for global deaths – each year, around 2.8 million adult deaths are linked to overweight and obesity. According to estimates, 23% of ischaemic heart disease burden, 44% of diabetes burden and 7-41% of cancer burden are attributable to obesity and overweight (WHO, 2014).
1.1. Global Obesity Trends
Representative data on childhood obesity is available for many developed countries, especially those in Europe and North America in addition to several developing countries (Lobstein, Baur & Uauy, 2004). Data on older children and adolescents is however limited in the case of developing countries. Overall, conclusions that can be derived from the available data, as summarized by Lobstein, Baur & Uauy, include:
Unequal distribution of the global prevalence of obesity –
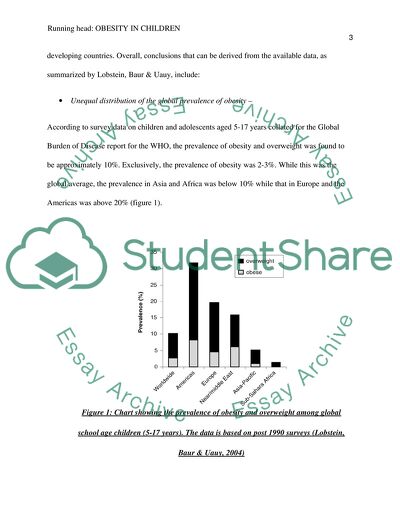
According to survey data on children and adolescents aged 5-17 years collated for the Global Burden of Disease report for the WHO, the prevalence of obesity and overweight was found to be approximately 10%. Exclusively, the prevalence of obesity was 2-3%. While this was the global average, the prevalence in Asia and Africa was below 10% while that in Europe and the Americas was above 20% (figure 1).
Figure 1: Chart showing the prevalence of obesity and overweight among global school age children (5-17 years). The data is based on post 1990 surveys (Lobstein, Baur & Uauy, 2004)
Rapid rise in childhood overweight –
The prevalence of overweight in children has been increasing at different rates and in different patterns in both developing and developed countries. A higher year-on-year increase is seen in European and North American countries. For instance, an approximate increase of 0.5% is seen per year in Brazil and the US and 1% per year in the UK, Australia and Canada in the past two decades.
High rates of overweight among the poor population of rich countries and the rich population in poorer countries –
Another interesting trend observed in global obesity prevalence is that in developed countries, children from poorer socio-economic groups are at a higher risk of obesity. On the other hand, children from higher socio-economic groups in developing countries have a higher prevalence of obesity.
In the US, surveys from 2009-2010 have shown that 16.9% children and adolescents are obese. The prevalence of obesity is higher in Hispanic and non-Hispanic black children as compared to non-Hispanic whites (Ogden et al., 2012). From the contrasting trends, it is hard to ascertain the causes and risk factors of obesity. In-depth epidemiological data, in addition to lifestyle and behavioral studies are essential for a more insightful understanding and estimation of the causes and risk factors involved in global obesity patterns among children.
1.2. Definition of Childhood Obesity
According to the CDC in US, overweight is defined as “having excess body weight for a particular height from fat, muscle, bone, water, or a combination of these factors” (CDC, 2013). Obesity is defined as “having excess body fat” (CDC). Different definitions of childhood obesity and overweight are used throughout the world (Ogden, 2012). However, the most widely accepted definition is related to body mass index (BMI) (McLennan, 2004). BMI implies weight (kg)/height2 (m). It is a simple index of weight for height and provides the most useful measure of obesity and overweight at the population level. It can be applied for both sexes and all ages but should be considered only as a rough guide as it may not necessarily tally with the same degree of fatness in different people. Children who are above the 85th percentile with respect to their BMI are considered as overweight and those above 95th percentile are considered obese. According to the WHO (2014) definition, BMI higher than or equal to 25 implies overweight and BMI higher than or equal to 30 implies obesity. In addition to BMI, anthropometry and waist circumference measurements are used as criteria for defining obesity and overweight. Both overweight and obesity result from caloric imbalance, when lesser calories are expended with respect to the total calories consumed. However, these are influenced by behavioral, lifestyle, environmental and genetic factors.
1.3. Assessment of Obesity
Obesity can be assessed by measuring body fat. According to Power et al. (as cited in Lobstein, Baur & Uauy, 2004),
An ideal measure of body fat should be accurate in its estimate of body fat; precise, with small measurement error; accessible, in terms of simplicity, cost and ease of use; acceptable to the subject; and well-documented, with published reference values… no existing measure satisfies all these criteria (p. 10).
As suggested, accurately estimating body fat is difficult and there is no universal consensus over the best assessment measure for obesity. In general, it is assessed using BMI or waist circumference (McLennan, 2004). Various methods can be employed for direct measurement of body composition in order to estimate the total fat mass in the body. These methods include magnetic resonance imaging (MRI), Air-displacement plethysmography, dual energy X-ray absorptiometry (DEXA), bioelectrical impedance analysis (BIA), computerized axial tomography (CT or CAT) and underwater weighing (hydro-densitometry) (Lobstein, Baur & Uauy, 2004). These measurement techniques are generally applied in tertiary care settings and for research. However, they may also be employed as a gold standard for the validation of body fat measurements done through anthropometric means.
Anthropometric measures of body fat include measurements of hip, waist and girth, measurement of skin fold thickness, indices such as the ponderal index (W H−3) or the Quetelets index (BMI or W H−2) that are derived from height and weight measurements, etc. (Lobstein, Baur & Uauy, 2004). These measurements are limited by the measurer’s skills and the accuracy of their results needs to be validated through direct adiposity measurements. All these methods have their own advantages and disadvantages and thus, one method can be used in supplementation with another. Direct measurement is generally used for validating results from anthropometric measurements. In case of large scale global surveys, however, it is not possible to use extensive direct measurements for each and every individual. Thus, most global trend data rely on anthropometric measures that are simple and easy to carry out.
1.4. Risk Factors and Causes for Childhood Obesity
Obesity results from ingestion of too much energy through food while expending too little energy through physical activity. The presently high rates of obesity in children has little association with genetic factors and more to do with lifestyle factors such as diet and exercise (Cameron, Hastings & Ellison, 2005). Investigations suggest that there has been a shift away from low fat and high fiber diets towards low fiber, high fat and high energy diets. There has also been an increase in sedentary activities replacing physical activities. For instance, television and video games have to some extent replaced sports; children commute to school in cars and buses instead of walking or cycling. In a previous study, Gortmaker et al. (1996) had shown that television viewing is a cause of increasing childhood obesity in the US. A strong dose-response relationship was observed between television viewing hours and overweight in 1990. They showed that over 60% of the incidence of overweight could be linked to excessive television viewing. However, computer games and television are not the sole reasons for increase in childhood obesity (Marshall et al. cited in Cameron, Hastings & Ellison, 2005). There has been a tremendous rise in the number of fast food outlets and there has also been an aggressive marketing of high-fat foods targeted at children. The fact that there are high rates of overweight in the poor population of rich countries and the rich population in poorer countries has already been mentioned in an earlier section. The rich urban population in developing countries considers eating at swanky fast food joints and restaurants as a sign of status. Moreover, they have lesser amounts of physical activity due to comfortable lifestyles as compared to the poor population. Because mostly, both the male and female parents are working in the urban population, they may rely on processed foods due to lack of time. This could be another reason for higher prevalence of obesity. In developed countries on the other hand, the inexpensive nature of fast foods may have led to its increased consumption by the poor population. All these are assumptions that have already been evaluated by many studies. It cannot however be conclusively said that these are the only reasons for the prevalence of obesity.
Genetic factors, medical syndromes and endocrine factors may also cause obesity in children (McLennan, 2004). While some of the risk factors for obesity are modifiable, others are not. Figure 2 lists both modifiable and non-modifiable risk factors for obesity. Non-modifiable risk factors include medical conditions, genetic predisposition, ethnicity, certain single gene abnormalities, high weight in the case of gestational age babies, and low weight with rapid catch up in gestational age babies. Modifiable risk factors include disordered eating, harmful lifestyle habits, television viewing and certain medical conditions.
Figure 2: Modifiable and non-modifiable risk factors for childhood obesity (McLennan, 2004, p. 35)
Studies on siblings, twins, extended pedigrees and nuclear families have shown that the chances of an individual being obese increase when his relatives are obese (Lobstein, Baur & Uauy, 2004). Moreover, the persistence of obesity from childhood into adulthood has also been linked with family obesity, especially when both the parents of a child are obese (Lake, Power & Cole, cited in Lobstein, Baur & Uauy, 2004). Studies have also shown that the impact of parental obesity on the weight of an individual in early adulthood is strongest from age 2 to 10 years. Subsequently by adolescence, the weight status of the child himself becomes a stronger determinant of the persistence of obesity into early adulthood (Whitaker et al., cited in Lobstein, Baur & Uauy, 2004). Therefore, it is suggested from research that while parental obesity is an important determinant of obesity in early childhood, it becomes a less important determinant above 10 years of age. Gene-environment interactions are also important risk factors in childhood obesity.
1.5. Consequences of Obesity
There are both long term and immediate effects of childhood obesity on the well-being and health of an individual. Obese children have a higher likelihood of being susceptible to cardiovascular disease associated risk factors such as high blood pressure and cholesterol. Studies on a population based sample of children in the 5 to 17 years age group showed that 70% of obese children have at least one cardiovascular disease risk factor (CDC, 2013). The likelihood of having prediabetes is also high in obese adolescents. In prediabetes, blood glucose levels are such that there is a high risk of developing diabetes. Other studies have also indicated that obese children have a greater risk of developing joint and bone associated problems. Other immediate effects include sleep apnea in addition to socio-psychological problems such as low self-esteem. Obesity in children in likely to persist into adulthood and therefore, in adulthood, they are at a higher risk of age-related health problems such as stroke, osteoarthritis, certain cancers, type 2 diabetes and heart disease. The cancers that are often linked with obesity and overweight include cancer of the colon, breast, esophagus, endometrium, gall bladder, kidney, pancreas, ovary, prostrate, cervix and thyroid. Obesity is also known to increase the risk of Hodgkin’s lymphoma and multiple myeloma (CDC, 2013). Obese or overweight children are also at risk of Type 1 diabetes, skeletal, circulatory and respiratory problems. Obesity is a pertinent cause of morbidity and mortality in adults and since childhood obesity often persists into adulthood, obese children are highly at risk. Studies estimate that upto 50% of obese children continue to remain obese in adulthood (McLennan, 2004). According to estimations by NAO in 1998, obesity resulted in more than 28,000 heart attack cases, over 250,000 Type 2 diabetes cases and 750,000 hypertension cases in adults (Cameron, Hastings & Ellison, 2005).
Several studies have shown that visceral adipose tissue is associated with lipotoxic fat. Elevated concentrations of leptin, low grade systemic inflammation and low levels of adiponectin are found in obese children, which are indicative of the possibility of metabolic syndrome (Lifshitz, 2008). Another interesting finding is that in children, there is a significant association between the incidence of asthma and excess weight (Lifshitz, 2008).
1.6. Economic Costs of Childhood Obesity
Increased prevalence of obesity increases the frequency of hospital treatment, increasing the pressure on the health services of a nation. Not only is there a direct burden on medical services but there are also other costs such as loss of educational opportunity, lost days of employment, etc. due to morbidity and mortality associated with obesity. Moreover, intangible costs such as psychological and social consequences also result from obesity (Lobstein, Baur & Uauy, 2004). Studies in various countries have investigated and estimated the direct costs of adult obesity (figure 3). According to these estimates, obesity accounts for around 2-7% of the total health care costs in developed countries.
Figure 3: Direct costs of adult obesity (Lobstein, Baur & Uauy, 2004, p. 30).
However, before drawing comparisons between these countries, it should be noted that the definitions of obesity vary across countries and the BMI cut-offs used in these definitions are different. Indirect costs of obesity as a result of loss or reduction in economic activity following premature death or illness attributable to obesity are also immense. In Australia, indirect costs have been estimated at AU$272m while in USA, they are as high as US$23bn. There is loss of productivity due to sick leaves and morbidity related reasons. Intangible costs associated with obesity also cannot be overlooked. One of the intangible costs associated with obesity is that of expenditure by families on weight loss programs. The quality of life of individuals is also affected through low self-esteem and other psycho-social factors, due which their productivity and contribution towards society and economic development of the country is also hampered.
Obesity is a growing cause of concern in both developed and developing countries. It is however a preventable issue. Therefore, large scale lifestyle, dietary and behavioral changes need to be implemented to lower the incidence of obesity. Other genetic and environmental factors also need to be studied in depth in order to understand how the risk factors of obesity can be averted.
References
Cameron, N., Hastings, G., & Ellison, G. (Eds.). (2005). Childhood Obesity: Contemporary Issues. Florida: CRC Press.
CDC. (2013, July 10). Childhood Obesity Facts. Retrieved from http://www.cdc.gov/healthyyouth/obesity/facts.htm.
Gortmaker, S. L., Must, A., Sobol, A. M., Peterson, K, Colditz, G. A., & Dietz, W. H. (1996). Television Viewing as a Cause of Increasing Obesity Among Children in the United States, 1986-1990. JAMA Pediatrics, 150(4), 356-362.
Lifshitz, F. (2008). Obesity in Children. Journal of Clinical Research in Pediatric Endocrinology, 1(2), 53–60.
Lobstein, T., Baur, L., & Uauy, R. (2004). Obesity in children and young people: a crisis in public health. Obesity Reviews, 5(s1), 4–85.
McLennan, J. (2004). Obesity in children - Tackling a growing problem. Australian Family Physician, 33(1/2), 33-36. Retrieved from http://softballone.com/rfe/obesity.pdf.
Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2012). Prevalence of Obesity and Trends in Body Mass Index Among US Children and Adolescents, 1999-2010. The Journal of the American Medical Association, 307(5), 483-490.
WHO. (2004). Childhood overweight and obesity. Retrieved from http://www.who.int/dietphysicalactivity/childhood/en/.
Read
More
sponsored ads
Save Your Time for More Important Things
Let us write or edit the literature review on your topic
"Obesity in Children"
with a personal 20% discount.
GRAB THE BEST PAPER
